

Summary
Factors that support radiation as a cause of the cancer spike

For comparison, the estimated average dose of radiation Hiroshima residents received is 210 milliSieverts. (Smart News/New York Times)
– A wide spectrum of cancers are appearing — in every part of the body.
– A wide variety of cancers found – 55 different types were put into the WTC cancer registry
- Radiation can cause many different types of cancers due to its ability to cause mutations in many different cells of the body; radiation is associated with all the cancers in the list of responder cancers (see below). As many as 55 different cancers were found in responders
– Radiation causes dose-dependent increase in cancer
- A dose of around 1000 milliSieverts cumulative dose causes 5 people out of 100 exposed people to develop cancers; 1000 milliSieverts is consistent with the radiation released from detonation of a nuclear device
– Unusual and rare cancers appearing
- Cancers that are usually seen in the elderly are showing up in relatively younger people, such as multiple myeloma. Childhood cases are also appearing. Cancers that are very rare are showing up with relatively higher frequency. For example, mesothelioma, a rare cancer, killed two workers, one in 2004 and another in 2006. This cancer usually has a long latency period of at least 25 years.
– Radiation causes mesothelioma
- thorium exposure (Thorotrast xray contrast medium – thorium dioxide) causes mesothelioma
- atomic energy workers have an increased chance of developing mesothelioma
- cases of mesothelioma in atomic bombing victims
- patients received radiation therapy have developed mesothelioma
- Mesothelioma associated with radiation can have short latency periods not seen in patients with asbestos-related mesothelioma.
– Characteristics of radiation-induced mesothelioma are different to asbestos-induced mesothelioma
- latency periods can be short with radiation-caused mesothelioma: one study reports a latency period of 0-4 years as well as longer latency periods – in the WTC cases, 1 WTC worker Deborah Reeve exposed died of mesothelioma in 2004 aged 41, and another worker died of mesothelioma in 2006. Asbestos.com
- mesothelioma of the epithelial type can be found; this type is not seen in asbestos-related mesothelioma
- mesothelioma of the peritoneum can occur in the radiation type.
– Arguments against asbestos
- asbestos causes only mesothelioma; 55 different cancers were found in responders
- association with leukemia not proven
- long latency period before mesothelioma appears when exposure to asbestos is involved. Minimum of 25 years in one study. Cancers among responders are appearing earlier than this.
- wearing a mask reduces exposure to asbestos significantly
– Cancer prevalence rates show a cancer spike
- There is a prevalence increase of 2-3x in certain age groups. For example, in September 11 responders aged 35-44 years of age, the prevalence rate was 24.54 per 1000. In the general population in 2013, males in the age group 30-39 years showed a cancer prevalence rate of 7.8 per 1000. In the general population, males aged 40-49 years, the prevalence rate was 15.9 per 1000.
– Radionuclides detected at WTC and 80 hot spots of radioactivity in Manhattan and Staten Island
- Elements in the radioactive decay chain of uranium, which is used to make nuclear explosives, were found in coatings of girders and dust in a study conducted by the USGS. Unusually high levels of barium and strontium were noted in particular. See tables below. In addition, high levels of tritium were found. After accounting for the fact that 20 million of liters of water had been poured into the “bath tub” of the WTC, the level of tritium that is calculated at the WTC is high and consistent with the detonation of a nuclear device. Scientists cite non-health damaging levels as evidence for lack of radiation. However, they fail to consider that before the decontamination procedures took place, such as flooding the basement of the WTC with millions of liters of water, which would have diluted the concentration of tritium, firefighters and police officers and other rescue personnel would have been exposed to the radiation released by tritium and from other radioactive substances in the area had nuclear weapons been used. Taking a reading of tritium at face value after decontamination has been done is not useful. A radiation survey performed by the GAO in 2005 found 80 radiation hot spots over Manhattan and in Staten Island. The actual spot on Staten Island has not been identified by GAO. In one media report, Fresh Kills is named. The 80 hot spots are not identified in detail in the GAO report. There is evidence that the evidence in Staten Island is being tampered with, in order to draw attention away from Fresh Kills landfill possibly. Initially, one radiation hot spot was detected, in 2005. In 2013, an additional radiation hot spot was discovered in Great Kills Park. In 2015, 1,200 radiation hot spots were found, in Great Kills Park. This increase in hot spots might indicate there is a deliberate attempt to obstruct the investigation into the presence of radiation hot spots in Staten Park by creating areas of radiation in Great Kills Park, which is done by deliberately planting radioactive material in that park. Some of the increase in cancers in Staten Island residents may have been caused by a deliberate seeding of radiation hot spots in Great Kills Park to mask the radiation in Fresh Kills.
Cancer elevations near residential locations close to Fresh Kills on Staten Island
- “Cancer Alley” near Fresh Kills landfill – “11 percent more people die of cancer than the rest of the city.” CBS New York
- Staten Island residents aren’t living as long as other boroughs. Life expectancy for men and women is lower than for four other boroughs and even for the whole state.
- Each week 48 people on Staten Island are diagnosed with cancer. Cancer is the second most frequent killer of residents.”The top four cancers on Staten Island [are] .. Female breast, prostate, lung and colorectal” SILive
- Staten Island has the highest breast cancer rate in the state. Voiz
- Staten Island is a lung cancer hot spot – 20% above state’s rate NYDailyNews
Most of the responders who would have received a very high dose would have been the police officers who came to the site first, after the explosions, to do search and rescue operations. Another group that would have received high doses of radiation would have been the firefighters who came to put out the fires after the towers had exploded and were also were present at the towers after their collapses to do rescue and recovery work. A third group who would have received high doses of radiation were the workers who worked at the Fresh Kills landfill site. Even if the first responders had not stayed for many days at the site, the level of exposure to radiation before decontamination could be started and when the dust cloud was at its most pronounced, darkening the air over Manhattan with dust particles, would have been at its highest. Those caught in the dust cloud when they escaped from the buildings would also have received a high dose of radiation.

Increase in cancers
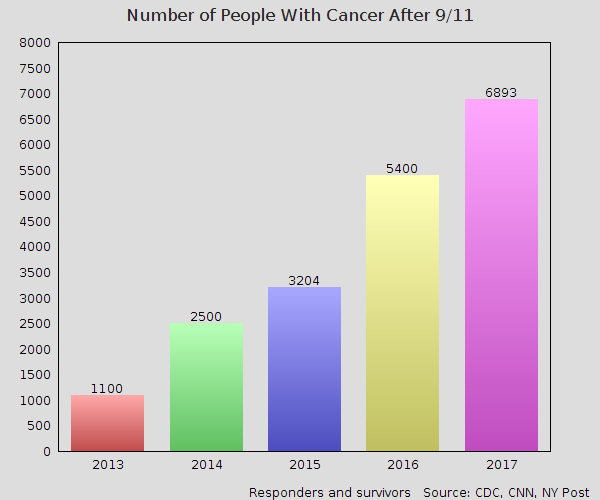
Total cancer certificates (responders and bystanders)
- In 2013: 1,100 (CNN)
- In 2014: 2,500 (link)
- In 2015 (February): 3,204 (CDC)
- In 2016: 5,400 (CDC, CNN)
- In 2017 (June): 6,893 (CDC)

From Factbox
Cancer spike

Cancer prevalence of total responders in WTC health program (2016)
The data is from CDC’s World Trade Center health program report of December 2016. Link: CDC–World Health Center Health Program Download pdf file: World Trade Center Health Program.
Summary of cancers in enrollees WTC Health Program (December, 2016)
– 5,105 responders out of 65,211 responders in program have cancer (8% or 1 in 12 responders have cancer)
– 867 survivors with cancer out of 10,121 survivors in program have cancer (8.5%)
– 5,972 enrollees out of 75,732 total enrollees have cancer (8%)
– 5,298 separate cancers in 5105 responders with cancer
– 890 separate cancers in 867 survivors with cancer
– 6,188 separate cancers in 5,972 enrollees with cancer
– 6,188 separate cancers in a population of 75,732 enrollees
Total number of cancer certifications: 6,188 as of Dec 31 2016; total number of enrollees with cancer: 5,972; total numbers of enrollees in program: 75,732, this data does not include deceased members (1,180 deceased responders, 86-95 deceased survivors, 216 deceased members who held cancer certification).
Some of these workers with cancer worked at the Shanksville and Pentagon sites. A total 401 responders who had worked at these sites were enrolled in the program. Since the number of these workers is relatively small compared to the number of people who worked at the WTC site or Fresh Kills landfill, radiation release is strongly suspected at these sites, and the number of people who worked at these sites who have cancer is unknown, these people are included in the calculations.
The prevalence of cancers in the total population of responders in the program in 2016 is 76.892952358 out of 1000 people
66,391 responders in the program
5,105 responders with cancer
Prevalence rate of cancer for the whole group of responders is 0.076892952358 or 76.892952358 people out of a population of 66,391 responders (for all age groups and both male and female responders). This includes those who worked at the Pentagon or Pennsylvania sites.
Cancer prevalence by age group for responders in program (2016)
Age group 35-44 years: cancer prevalence rate is 24.54 per 1000 people
Age group 35-44 years: 210 with cancer. No. of responders aged 35-44 years of age were 8,557.
Prevalence rate of cancer in this age group of 0.024541311206199 or 24.541311206199 per 1000 people in this age group exposed to the WTC site or Fresh Kills landfill site have cancer.
Age group 45-54 years: cancer prevalence rate is 53.7655 out of 1000 people
Age group 45-54 years of age: 1395 cancers, 25,946 responders in this age category were enrolled in the program
Age group 55-64 years: cancer prevalence rate is 103.991751362498 out of 1000 people
Age group 55-64 years of age: 2118 cancers, 20,367 responders in this age group enrolled in the health program.
Age group 65-74 years: cancer prevalence rate is 155.758426966292 per 1000 people
Age group 65-74 years: 1,109 cancers. 7120 responders of this age group enrolled. 0.155758426966292
Age group >74 years: cancer prevalence rate is 158.6651053864 per 1000 people
Age group >74 years: 1708 people enrolled in this age group. 271 cancers.
The prevalence rate does not include responders in the program who died, 1,180, nor the responders who died before the program started nor the responders who chose not to enrol in the program. 216 responders in the program with cancer have died according to the site. However, it does not give more information about these people, such as what year they died in and what age group they were in. These people were not included in the calculations above. The prevalence rate is probably an underestimation for these reasons. It only counts one cancer per individual.
Cancer prevalence in the US general population (2013)
In the 2013 SEERS data for cancer prevalence of all cancer sites, American males showed cancer prevalence of the following rates*:
Males age 20-29 years: cancer prevalence rate of 4.048186980433 per 1000 people
Males age 20-29 years: 89,810 cases of cancer. Prevalence rate is 0.004048186980433 or 4.048186980433 per 1000 people. Combining census data from 2010 and 2013 gives the total number of males in this age group in 2013 as 22,185,245 males. 0.142637854678278 of the male population in 2010 were in this age group, so in 2013, this age group comprised of 22,185,245 males
Male age 30-39 years: cancer prevalence rate of 7.8 per 1000 males
Male age 30-39 years: 160,506 cases of cancer. 13.2022314787262% of the male population or 20,534,152 males were in this age group in 2013 (combining 2013 and 2010 data). This gives a 160,506/20,534,152 prevalence rate for this age group or 0.007816539 prevalence of cancer in people aged 30-39 years in 2013 (7.8 out of 1000 males aged 30-39 years would have a cancer)
Male age 40-49 years: cancer prevalence rate of 15.902281881571 per 1000 males
Age 40-49 years: 352,035 cases of cancer in males. According to the 2010 census data, 0.142330170445342 of the male population are in this age group. This is 22,137,389 males.
Male age 50-59 years: cancer prevalence rate of 43.904371823346 per 1000 males
Age 50-59 years: 920,363 cases of cancer in males. 0.134778912130469 of the total males were in this age group in 2010. This gives an estimate of 20,962,901 males in this age group in 2013.
Male age 60-69 years: cancer prevalence rate of 124.515301349089 per 1000 males
Age 60-69 years: 1777405 cancers in total, of all types. According to the 2010 census data, 0.091777080666695 of total males were in this age group. This gives an estimated figure of 14,274,591 males in this age group in 2013.
Male age 20-69 years: cancer prevalence rate of 32.97010644 per 1000 males
3,300,119 cancers in males aged 20-69 years out of a total population of 100,094,278 males aged 20-69 years.
*The cancer counted only includes the first malignant primary cancer. The male population data above is based on the following data from the US Census Bureau that shows the total population of the USA in 2013 was an estimated 316,129,000. Wikipedia: Demography of the US . The age demographics data is for 2010 is here: Census-Gov. The male:female sex distribution is assumed to be 49.2 to 50.8% (stats for 2010, US Census bureau). The number of total males in the age groups is based on combining the data from these sources.
Note: These prevalence rates are only rough estimates. The comparisons are therefore only estimates. The total number of responders exposed to the dust and debris of the WTC and at Fresh Kills landfill would have to be determined exactly. The total sex ratio breakdown of the different cancers among the responders would have to be determined. The age adjusted rates for cancer incidence that match the age groups of the general population would have to be provided. More accurate determinations of the male to female ratio of cancers in the WTC program population and a comparison of these ratios to the ratios of male to female prevalence of cancers would have to be calculated. The number of people who died in that year would have to be obtained and more information about these people such as what age groups they were in. The number of people with cancer who did not enrol in the program would improve the accuracy as well. The number of people with cancer who had died before the program started would also be helpful.


World Trade Center Health Program
This was a program established to provide health care and monitoring for people who have been affected by the September 11 attacks.
It also provides treatment and screening for people who worked or lived close to the Manhattan disaster area on September 11 or the months that followed it. This group of people are called Survivors.
The WTC Health Program was established by the James Zadroga 9/11 Health and Compensation Act of 2010. In 2015, the Program was reauthorized until 2090.
The pdf file for WTC Health Program at a Glance 2016 can be downloaded here: World Trade Center Health Program
Responders
According to the Centers for Disease and Prevention September 11 health program, responders are:
“emergency responders, recovery and cleanup workers, and volunteers who helped at the World Trade Center, the Pentagon, and the crash site near Shanksville, Pennsylvania.”
Gender of members

65,211 responders in total, 10,121 survivors
WTC Health Program Member Age Distribution

Members with certifications by Zadroga Act – categories of conditions

Top 10 certifications

5298 cancers in 5105 responders with cancer
890 cancers in 867 survivors with cancer
total number of enrollees with cancer:
6188 cancers in 5972 enrollees with cancer
6188 cancers in a population of 75,732 enrollees
5972 members with cancer in a population of 75,732 enrollees
Total number of cancer certifications: 6188 as of Dec 31 2016; total number of enrollees with cancer: 5972; total numbers of enrollees in program: 75,732
Cancer age distribution

5275 cancers in 5105 responders, 78.2843385 per 1000 responders have cancer
5972 members (responders and survivors) hold
Survivors hold
Types of members

Types of cancers – top 15 cancers

SEERS: US prevalence-invasive cancers in 2013:

Prevalence of cancers according to age group in US total population in 2013
Prevalence of breast cancer etc in 2013

Population of USA in 2013

Total population of the USA in 2013 estimated to be 316,129,000 (Wikipedia)
From City Lab:
14 Years Later, Here’s What We Know About 9/11 and Cancer
The link has become increasingly clear—just as victim funding is set to expire
ARIA BENDIX Sep 10, 2015
50 cancers were added to the list of cancers eligible for compensation
“In 2011, 10 years after the attacks, Congress reactivated the fund via the James Zadroga 9/11 Health and Compensation Act—named after an NYPD officer and first responder who died of respiratory disease—in addition to establishing a new World Trade Center Health Program. Two years later, officials finally added 50 different types of cancer to the list of diseases eligible for compensation.” City Lab
Health department found no clear association between cancer and the debris at the World Trade Center
“In one of the most comprehensive studies of its kind to date, the New York City Health Department found no clear association between cancer and the debris at the World Trade Center site. The study, published in 2012 in the Journal of American Medical Association, observed 55,778 New York residents who were present at the World Trade Center on the day of the attacks and had enrolled in the World Trade Center Health Registry. Among those observed, 1,187 had been diagnosed with cancer by the time of the study.” City Lab
Radiation as a cause was not examined in the study. Only PAHCs, asbestos and similar toxins were examined. Rationale for not looking at radiation was based on no radionuclides found. However, this report shows there were many radionuclides found in the dust and girder leachates of the WTC.
When comparing this number to all New York state residents, the study found an increased risk of prostate cancer, thyroid cancer, and myeloma, but ultimately could not connect the diagnoses to 9/11 due to a lack of statistical significance. But the causes they looked at in detail were PAHCs and other toxins. They did not look at radiation in depth.
In 2013, Environmental Health Perspectives published a study that found more conclusive evidence of a link between cancer and 9/11. Of the 20,984 participants—all World Trade Center rescue and recovery workers—552 were diagnosed with cancer between 9/11 and December 2008. Those who had been highly exposed to carcinogens and pollutants were more likely to be diagnosed. In addition, the study’s authors were surprised to find higher levels of thyroid and prostate cancer than they had originally anticipated City Lab
Higher levels of thyroid and prostate cancer can be caused by exposure to radiation. These cancers are usually not caused by non-radiation environmental toxins.
There’s no doubt in his mind that we will see a sharp increase in 9/11-related cancers over the next 30 years. City Lab
The cancer rate seems to be increasing by 1,200 every year. In 2013, the number of cancer cases was 1,100. In 2014, the cancer cases was reported to be 2,500. In 2016, the number of cancer cases was found to be 5,400. 5972 members in the WTC health program held cancer certificates (had cancer diagnoses). This figure does not include the 216 who held cancer certificates who had died.
As of last year, there have been more than 2,500 reported cancer cases among World Trade Center rescuers and responders. City Lab
In 2014, it was reported that there were 2,500 reported cancer cases. Not all responders or survivors enrolled in the World Trade Center so the cancer figures are probably all underestimates.
These cancers span the full gamut—thyroid, prostate, lung, pancreatic, leukemia, multiple myeloma. The list goes on, though Flores thinks it wise to focus on the big three: esophageal cancer, lung cancer, and mesothelioma. City Lab
The gamut of cancers run the whole range and include even rare cancers and childhood cancers. This cancer profile can be seen with radiation. Esophageal cancer can develop through ingestion of radioactive particles through the oral route and lung cancer can develop through the inhalation of radioactive particles into the respiratory system.
World Trade Center Health Program; Addition of Certain Types of Cancer to the List of WTC-Related Health Conditions
Quote
|
AGENCY: Centers for Disease Control and Prevention, HHS. B. Summary of Major Provisions This rule modifies the List of WTC-Related Health Conditions in 42 CFR 88.1 to add the following conditions (types of cancer identified by ICD-10 code are specified in the discussion below): ▪ Malignant neoplasms of the lip, tongue, salivary gland, floor of mouth, gum and other mouth, tonsil, oropharynx, hypopharynx, and other oral cavity and pharynx |
The following cancers have been added to the list of WTC-related conditions.
|
The Administrator adds the specific types of cancers in the list below to the List of WTC-Related Health Conditions in 42 CFR 88.1.” ▪ Malignant neoplasms of the lip [C00], tongue [C01, C02], salivary gland [C07, C08], floor of mouth [C04], gum and other mouth [C03, C05, C06], tonsil [C09], oropharynx [C10], hypopharynx [C12, C13], other oral cavity and pharynx [C14] (Method 3) |
Association between radiation and mesothelioma
Summary
Mesothelioma has been linked to radiation exposure. The latency period in some studies of radiation and development of mesothelioma has been as short as 0-4 years (prostate cancer study). In one study of asbestos exposure and mesothelioma, the latency period ranged from 25 to 68 years.
Long latency period of mesothelioma development and asbestos exposure
One study done on shipyard workers in Italy showed long latency periods in mesothelioma cases caused by asbestos exposure
The latency periods observed in the present mesotheliomas showed extreme variations, from 25 to 68 years. The mean latency period was superimposable to that observed in large series of mesotheliomas among shipyard workers in the Trieste-Monfalcone area. [18]
Mesothelioma.com: Resources for patients
One report found that as many as 25-33% of cases in the US and Canada are not related to asbestos exposure
As a matter of fact, a 1980 study (McDonald and McDonald) of patients in the U.S. and Canada determined that somewhere between 25 percent and 33 percent of all cases were not related to asbestos exposure.
This report cites cases where radiation is considered to have caused mesothelioma. One case involves exposure to radiation from atomic bombing.
In 1995, the first case of mesothelioma believed to be associated with the dropping of the atomic bomb in Nagasaki was diagnosed. A report on this case, penned by Masami Mizuki, Keiko Yukishige, Yasuharu Abe, and Tomiyasu Tsuda, and published in the journal Respirology in September 1997, suggested that combined exposure to atomic radiation and asbestos (the patient worked for 2 years as a shipbuilder at a munitions factory) is associated with an increased incidence of mesothelioma.
Another case involves exposure to radiation during radiation therapy for cancer.
Throughout the world, a number of cases of mesothelioma with no apparent connection to asbestos have been diagnosed. As a matter of fact, a 1980 study (McDonald and McDonald) of patients in the U.S. and Canada determined that somewhere between 25 percent and 33 percent of all cases were not related to asbestos exposure. Doctors found this perplexing at first, but with some in-depth research and several official studies, scientists and medical professionals were able to determine that some of these pleural mesothelioma patients had other factors in common. Exposure to radiation was one of those factors.
Another study showed that patients who had Hodgkin’s disease who were treated with radiotherapy developed mesothelioma.
Several dozen cases of mesothelioma following radiation therapy for Hodgkin’s disease have been discovered. A 2005 study entitled “Clinical Course of Thoracic Cancers in Hodgkin’s Disease Survivors” (P. Das, A.K. Ng, M.A. Stevenson, and P.M. Mauch) definitively determined that Hodgkin’s disease patients who were treated with radiation therapy have a high incidence of mesothelioma disease.
A study found mesothelioma was linked to radiation therapy to the breast and chest area
In some cases, peritoneal mesothelioma has also been linked to radiation therapy for breast cancer or any other cancers that may have included radiation delivered to the chest area.
A connection was made to radioactive substance thorium dioxide, a radioactive substance that used to be used alongside xrays to make a diagnosis.
Other research makes a connection between mesothelioma cancer and thorium dioxide, a radioactive substance that was used along with conventional x-rays to diagnose certain conditions. Thorium dioxide was used abundantly from the 1920s until the 1950s.
Working in atomic power plants and being exposed to low levels of radiation for long periods is believed to be connected to mesothelioma, a rare disease. This leads clinicians to state that radiation is one of the risk factors to consider when mesothelioma is diagnosed.
Wherever radiation is present, there seems to be a potential connection to mesothelioma. Throughout the last few decades, several individuals currently or formerly employed at atomic energy plants have been diagnosed with this rare cancer, in these instances thought to be caused by constant exposure to low level radiation. (Ionizing radiation: A risk factor for cancer; JE Goodman et al, 2009) The authors concluded that, considering the low rate of mesothelioma in the general population, the increased risk of the disease among radiation-exposed individuals, including those who work at atomic power plants, is significant and should be duly noted. Mesothelioma
Mesothelioma developed in patients with non-Hodgkin lymphoma of 25 years, testicular carcinoma patients, breast cancer who had been treated with radiation therapy
Radiation therapy has also been implicated as a possible cause of mesothelioma. In a study of 77,876 non-Hodgkin lymphoma patients under the age of 25 treated with radiation only, 18 developed mesothelioma.6 In a study of 40,000 testicular cancer patients treated with radiation during the years 1943-2001, 10 developed mesothelioma without any obvious asbestos exposure.7 A review of 22,140 breast cancer patients treated with radiation on 1 of 11 National Surgical Adjuvant Breast and Bowel Project clinical trials showed that 3 developed mesothelioma.8 NCBI-National Institutes of Health
In a study of non-Hodgkins patients, irradiated patients had a higher risk of developing mesothelioma than non-irradiated patients.
Irradiated patients had excess risk for sarcomas, breast cancers, and mesothelioma compared with unirradiated survivors (P < .05). NCBI-National Institutes of Health
Irradiation of prostate cancer patients is linked to mesothelioma. Latency periods observed can be as short as 0-4 years
Four hundred and seventy-one mesothelioma cases (93.6 % pleural) occurred in 3,985,991 person-years. The IRR [incidence rate ratios] of mesothelioma was increased for subjects exposed to EBRT (1.28; 95 % CI 1.05, 1.55) compared to non-irradiated patients, and a population attributable fraction of 0.49 % (95 % CI 0.11, 0.81) was estimated. The IRR increased with latency period: 0–4 years, IRR 1.08 (95 % CI 0.81, 1.44); 5–9 years, IRR 1.31 (95 % CI 0.93, 1.85); ≥10 years, IRR 1.59 (95 % CI 1.05, 2.42). Despite the fairly strong evidence of association with EBRT, the population attributable rate of mesothelioma was modest—3.3 cases per 100,000 person-years. The cumulative incidence of mesothelioma attributable to EBRT was 4.0/100,000 over 5 years, 24.5/100,000 over 10 years, and 65.0/100,000 over 15 years. NIH
Latency periods that were studied were 0-4 years, 5-9 years, and ≥10 years
20% of patients with mesothelioma have no exposure to asbestos
In addition, about 20% of the patients have no history of asbestos exposure even after detailed assessment. Archives of Pathology
Therapeutic radiation linked to mesothelioma with latency periods ranging from 7-50 years
THERAPEUTIC IRRADIATION
Ionizing radiation is a recognized human carcinogen and an established risk factor for several different types of cancers including hematologic malignancies and solid tumors. Cases of MM of the pleura, peritoneum, and pericardium have been reported in humans after therapeutic irradiation and thorium dioxide administration. The latency period has ranged from 7 to 50 years, with a mean of 21 years and an equal male to female ratio.40–49 The evidence linking ionizing radiation to the development of MM can be looked at from 3 epidemiologic viewpoints: (1) patients exposed to thorium dioxide (Thorotrast), a diagnostic x-ray contrast medium; (2) patients receiving radiation therapy for cancers such as Wilms tumor, breast cancer, malignant lymphoma, and testicular malignancies; and (3) atomic energy workers chronically exposed to lower levels of radiation.50
Thorium dioxide is insoluble and once injected, cannot be excreted. It is therefore retained within a variety of tissues but continues to decay, emitting mostly α particles. Exposure to Thorotrast has been found to increase the risk for pleural and peritoneal MM in cohorts in Denmark, Sweden, Japan, Germany, and the United States.51–56 The cohort studies have generally examined the risks of MM between the general population and patients undergoing the same radiographic procedure with and without Thorotrast. The results of these studies are consistent in showing an elevated risk for pleural and peritoneal MM with radiation exposure; since asbestos exposure was unlikely to have been different among the treatment groups, it is not likely to have been a confounding factor in these studies.51
The evidence linking therapeutic radiation to the development of MM has come from case reports41–45,47,49,56 and several large-scale retrospective cohort studies.55 The latter have used population-based registries, such as the Surveillance Epidemiology and End Results data, and second primary cancers in individuals with the same type of primary cancer, to examine the occurrence of MM after exposure to therapeutic radiation for treatment of several different types of cancer.44,57–64 De Bruin et al64 found that among 2567 5-year survivors of Hodgkin lymphoma, the risk for malignant mesothelioma was almost 30-fold for patients treated with irradiation, as compared to the general population. Archives of Pathology
Mesothelioma of the epithelial type more common in patients with radiotherapy
Conclusions.— Patients with mesothelioma and hematologic malignancies with a history of radiation tended to be younger, had a longer interval from diagnosis of hematologic malignancy to that of mesothelioma, had a longer survival period, and were more likely to have the epithelial variant compared with patients without radiotherapy. Archives of Pathology
Asbestos not associated with hematological malignancies
A number of case reports have suggested a relationship between asbestos exposure and hematologic malignancies, including non-Hodgkin lymphoma, leukemia, and multiple myeloma/plasmacytoma.2–6 Whereas Ross et al7 reported that primary large cell lymphomas of the gastrointestinal tract and oral cavity were related to asbestos exposure in a case-control study, subsequent studies failed to confirm those findings.8–10 Furthermore, epidemiologic studies have generally failed to confirm an increased risk of hematologic malignancies in association with asbestos exposure.11–15 Consequently, asbestos is not regarded as a human lymphoid carcinogen, although asbestos fibers have been reported in lymph nodes and bone marrow.16–18 Although hematologic malignancies have been reported in experimental animals exposed to asbestos via inhalation or inoculation, no statistically increased incidence of those malignancies was detected.19–21 Archives of Pathology
Ionizing radiation lined to mesothelioma in animals and humans
The following were found to be risk factors for developing mesothelioma
- Plutonium (caused mesothelioma in rats)
- Thorotrast (thorium dioxide) an xray contrast medium
- Working at nuclear facilities
- Radiotherapy for primary malignancies – patients at risk include those treated for Hodgkin lymphoma, non-Hodgkin lymphoma, testicular cancer and breast cancer
Ionizing radiation has been linked to malignant mesothelioma both in animals and in humans.23–39 Sanders and Jackson23 reported that 27% of rats treated with plutonium particles developed malignant mesotheliomas and concluded that the pathogenesis of malignant mesotheliomas induced by radioactive particles seemed similar to that of mesothelioma after intracavitary administration of asbestos. Several forms of ionizing radiation have been related to the development of malignant mesothelioma, including administration of Thorotrast (an x-ray contrast medium),24 working at nuclear facilities,25–26 and radiation treatment for first primary malignancies.27–39Case reports29–33 of patients developing malignant mesothelioma within or adjacent to radiation fields were followed by large-scale retrospective cohort studies, using data from the US National Cancer Institute’s Surveillance, Epidemiology, and End Results program, indicating an increased risk of malignant mesothelioma in patients receiving radiotherapy for primary malignancies. Patients at risk included those treated for Hodgkin lymphoma, non-Hodgkin lymphoma, testicular cancer, and breast cancer.34–39
Cancer Alley – Fresh Kills landfill

- “Cancer Alley” near Fresh Kills landfill – ““Apparently, 30 percent more people die of heart disease on Staten Island than the rest of the city as a whole and 11 percent more people die of cancer than the rest of the city.” CBS New York
- Staten Island residents aren’t living as long as other boroughs – “The borough, in 2009, had the highest death rates per 100,000 people among the five boroughs for heart disease, cancer, pneumonia and chronic lower respiratory disease, Health Department statistics show.”
- Each week 48 people on Staten Island are diagnosed with cancer. Cancer second most frequent killer of residents.”The top four cancers on Staten Island have remained steady over time: Female breast, prostate, lung and colorectal…In the five-year period from 2005 to 2009, a whopping 6,456 cases of these four cancers were reported, with female breast (1,788 cases) in first place, closely followed by prostate (1,775 cases), and then lung cancer with 1,679 cases and colorectal with 1,214 cases.” SILive
- Staten Island has the highest breast cancer rate in the state. Voiz
- Staten Island is a lung cancer hot spot – 20% above state’s rate NYDailyNews
- 1.62 million tons of debris from the WTC were dumped on Fresh Kills landfill
- ‘Hundreds of federal agents, firefighters, police officers, and blue-collar workers plowed through up to 9,000 tons a day for 10 months at “the Hill”‘ (US News & World Report – dead link)
- Steel was sent off to be recycled – spread of radioactivity to the general community “The swatches of clothing, the driver’s licenses, and the family pictures culled from the refuse now sit at police headquarters, waiting to be claimed. Also gone are the stacks of crushed vehicles, more than 1,300 in all; some of them have been shipped to museums, while others have been recycled into steel.” (US News & World Report – dead link)
- More than 1.4 million tons of debris were buried in Fresh Kills in “large graves”. This would contain the radioactivity to some degree (US News & World Report – dead link)

USGS Report
Download pdf file: USGS Spectroscopy Lab – World Trade Center USGS Chemistry Table
Link: USGS: WTC Chemistry Table
Gallium
Plutonium–gallium alloy (Pu–Ga) is an alloy of plutonium and gallium, used in nuclear weapon pits, the component of a nuclear weapon where the fission chain reaction is started. This alloy was developed during the Manhattan Project. (Wikipedia)
Thallium
- Thallium-208 is a decay product of uranium-232.
Summary
Radionuclides were found in the dust of the WTC site and beam coating samples. Many fission products in the radioactive decay chain were found in the analysis. Also, gallium, which is an element used in the making of nuclear bombs, was found.
Strontium and barium were notably for their high elevations in leachates. These are not normally found in the environment in such high amounts. Scientists, who were surprised that strontium and barium were found at such high levels, postulated that the leaching process somehow introduced an artifact that produced these higher levels. However, such elevated findings are not abnormal if the possibility of the detonation of a nuclear device is considered, as elevated levels of these radioactive elements are normally found after nuclear tests.
In addition, the consistency of the findings of the various samples taken indoors and outdoors, as well as the consistency of the results among samples taken both indoors and both outdoors, that show the presence of many radionuclides found in the decay chain of uranium as well as elements used in the manufacture nuclear weapons, indicates that nuclear explosions took place at the WTC.
The finding of radionuclides in WTC dust and beam coating samples is supported by the finding of elevated radiation levels in Staten Island, the location of the Fresh Kills landfill site, in a helicopter radiation survey conducted by the GAO in 2006. 2006 is the year when the increase in cancer incidence began to show. This may have prompted officials to perform the survey. The exact location of the Staten Island site was not identified in the report. However, two officials, one from the NYPD and another, Republican Congressman Fosselli, say that the hot spot is Great Kills. This has not been confirmed to have been the same hot spot identified in the GAO Report. It’s possible that sayanim who knew that the radiation survey would be done planted radioactive materials in Great Kills Park to divert attention away from Fresh Kills, and other people within the government collaborated or were used unwittingly to mislead the public. More on this in the GAO Radiation Survey section.
Both of these findings: elevated radionuclides, including many radionuclides in the radioactive decay chain of uranium, and elevated radiation levels in 80 hot spots over Staten Island and WTC site, support the hypothesis that nuclear devices were detonated at the WTC site on September 11, releasing radioactive elements and radiation into the environment. The increase in cancer prevalence, involving a wide variety of cancers, including rare and unusual cancers, also supports the hypothesis that a nuclear explosion(s) occurred at the WTC site.
For more information about radionuclides, including tritium, go to the Radionuclides section and look at the GAO Radiation Survey section.
Radionuclides found in outdoor samples:
Sample 1
Barium, strontium, cerium, yttrium, nickel, lanthanum, antimony, molybdenum, thorium, rubidium, cobalt, niobium, uranium, cadmium, gallium, beryllium, cesium, bismuth, thallium.
Sample 2
Barium, strontium, cerium, yttrium, nickel, lanthanum, antimony, thorium, rubidium, cobalt, niobium, uranium, cadmium, gallium, beryllium, cesium, bismuth, thallium
Sample 3
Barium, strontium, cerium, yttrium, nickel, antimony, molybdenum, thorium, rubidium, cobalt, niobium, uranium, cadmium, gallium, beryllium, cesium, bismuth, thallium
Radionuclides found in indoor dust and girder coatings samples
Sample 1
Barium, strontium, cerium, yttrium, nickel, antimony, molybdenum, thorium, rubidium, cobalt, niobium, uranium, cadmium, gallium, beryllium, cesium, bismuth, thallium
Sample 2
Barium, strontium, cerium, yttrium, nickel, antimony, lanthanum, antimony, molybdenum, thorium, rubidium, cobalt, niobium, uranium, cadmium, gallium, beryllium, cesium, bismuth, thallium
Total list of uranium fission products and radionuclides used in manufacture of nuclear weapons
Barium, strontium, cerium, yttrium, nickel, lanthanum, antimony, molybdenum, thorium, rubidium, cobalt, niobium, uranium, cadmium, gallium, beryllium, cesium, bismuth, thallium
Chemistry Tables showing data for elements analyzed in WTC dust and beam samples
TABLE
Radionuclides and elements used in nuclear weapons manufacture shown in color in table. Note the original report does not show the colored highlighting.
Outdoor dust samples

Figure 1

Figure 2: Barium, strontium, cerium, yttrium, nickel, lanthanum, antimony, molybdenum, thorium, rubidium, cobalt

Figure 3: Niobium, uranium, cadmium, gallium, beryllium, cesium, bismuth, thallium.
Outdoor dust samples

Figure 4: Barium, strontium, cerium, yttrium, nickel, lanthanum, antimony

Figure 5: Thorium, rubidium, cobalt, niobium, uranium, cadmium, gallium, beryllium, cesium, bismuth, thallium
Outdoor dust samples

Figure 6: Barium, strontium, cerium, yttrium, nickel

Figure 7: Antimony, molybdenum, thorium, rubidium, cobalt, niobium, uranium, cadmium, gallium, beryllium, cesium, bismuth, thallium
Indoor dust samples and girder coatings

Figure 8: Barium, strontium

Figure 9: cerium, yttrium, nickel, antimony, molybdenum, thorium, rubidium, cobalt, niobium, uranium, cadmium, gallium, beryllium, cesium, bismuth
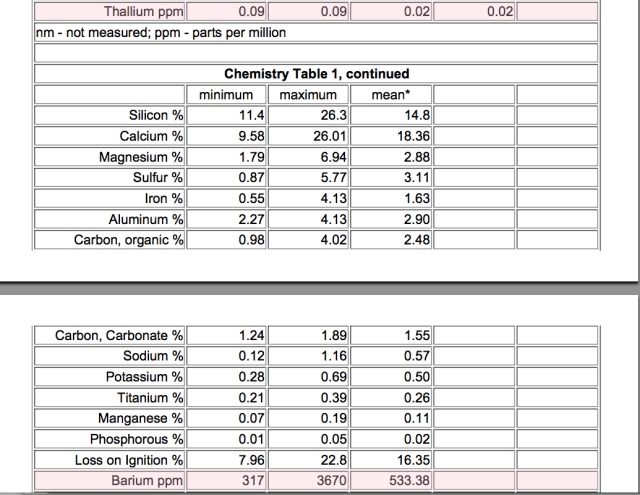
Figure 10: Thallium. Sample 2: Barium

Figure 11: Strontium, cerium, yttrium, nickel, antimony, lanthanum, antimony, molybdenum, thorium, rubidium, cobalt, niobium, uranium, cadmium, gallium, beryllium, cesium, bismuth, thallium

Figure 12 LINK: WTC Chemistry Table DOWNLOAD: USGS WTC Chemistry Table
__________________________________________________________________________
2011 article about a study done on firefighters and cancer – increase in cancerr rates admitted for the first time by health authorities
– Firefighters who worked at WTC on September 11 getting cancer at a higher rate than firefighters who worked before 9/11
– 7-year study on 9/11 firefighters said there was an “unusual” increase in 9/11 firefighters
– Some cancers in 9/11 firefighters are ‘bizarrely off the charts’
– Cancer cases across ‘all ranks’ of the FDNY who worked at Ground Zero are ‘up significantly’
– Cites unusual rises in leukemia, non-Hodgkin’s lymphoma and multiple myeloma.
– The report also states increases in esophageal, prostate and thyroid cancers.
– Officials still insist there is no scientific proof that Ground Zero smoke and dust caused cancer
9/11 NUKE DEMOLITION PROOF: Firefighters Radiation Cancers “Off the Scale”By GPD on April 4, 2011 RADIATION CANCERS KILL 345 SO FAR 9/11 FIREFIGHTERS ARE GETTING CANCER AT A FASTER RATE THAN OTHERS, CHIEF MEDICAL OFFICER REVEALS By Daily Mail Reporter Firefighters who recovered bodies at Ground Zero are developing cancer at a faster rate than those who worked before the atrocity, medical officials have revealed. A seven-year study by the New York Fire Department has claimed that there are ‘unusual rises’ in the number of cancer cases among firefighters who worked in the aftermath of 9/11. Some types of cancer among 9/11 firefighters are even ‘bizarrely off the charts’, according to sources who have seen the as-yet-undisclosed federal-funded study. Dr. David Prezant, the Fire Department’s chief medical officer, has reportedly said that cancer cases across ‘all ranks’ of the FDNY who worked at Ground Zero are ‘up significantly’. It is thought that the report – due to be officially disclosed in time for the 10th anniversary of the terror attacks in September – cites unusual rises in leukemia, non-Hodgkin’s lymphoma and multiple myeloma. The report also states increases in esophageal, prostate and thyroid cancers. Although officials have yet to confirm the increase, sources who attended a recent steering-committee meeting said Dr. Prezant’s report will document the cancer increase. One source told the New York Post: ‘The only conclusion that could have been reached was that there was an increase in the cancer rate for firefighters after 9/11.’ Minutes of the meeting quote Prezant as saying that ‘we have completed our seven-year cancer study’ and that he planned to present it to the fire unions. A doctor from the National Institute for Occupational Safety and Health is said to have asked Dr. Prezant: ‘In the past, you mentioned about the rates before being somewhat similar — what led to the change that you noted the increase?’ Prezant said researchers have compiled medical records for three years and had access to state cancer registries, though New York’s is three years behind. Dr. Prezant reportedly told the group: ‘Those things keep adding cases The report would be the first to document a cancer-rate increase among rescue and recovery workers. The city recently settled lawsuits by 10,000 WTC workers, more than 600 of whom have developed cancer. But officials have so far insisted there is no scientific proof that Ground Zero smoke and dust caused cancer. An FDNY spokesman gave a statement for Dr. Prezant, saying: ‘The study is ongoing, and no conclusions have been reached on whether cancer rates have increased for firefighters.’ But fire union bosses in New York have expressed their concern about the findings. Al Hagan, head of the fire-officers union, told the New York Post: ‘I’m led to believe that the numbers for those cancers across all ranks in the Fire Department of people who worked at Ground Zero is up significantly, and we’re all very concerned about it, as are our families.’ Steve Cassidy, president of the firefighters union, said Ground Zero’s ‘toxic stew’ has proven lethal. He said: ‘It’s a fact that New York City firefighters are dying of cancer in record numbers. ‘We have buried 10 firefighters in just the last 15 weeks, seven with cancer. On Sept. 10, 2001, they were young, healthy firefighters.’ In 2007, doctors at Mt. Sinai Medical Center, which monitors World Trade Center rescue workers, noted blood cancers like multiple myeloma, which normally strikes in the 60s or 70s, were being found in relatively young officers. The New York state Health Department has confirmed that 345 Ground Zero workers have died of various cancers as of June 2010. |
___________________________________________________________________________
Marcy Borders, iconic “Dust Lady”, dies at age 42 years of stomach cancer in 2015

Marcy Borders, the Dust Lady, was caught in a dust cloud when she escaped from the 81st floor of the North Tower after the North Tower had been hit by a plane. She managed to escape just as the South Tower came crashing down. She contracted stomach cancer, probably secondary to the radiation, and died in 2015.

Marcy Borders, 42, known as the ‘Dust Lady’, had attributed her stomach cancer – diagnosed in April 2014 – to the after-effects of the attack in 2001 which claimed 2,753 lives.
The mother-of-two, who is believed to have died on Monday night according to her family’s social media posts, blamed her illness on inhaling dust particles: “I’m saying to myself ‘Did this thing ignite cancer cells in me?
“I definitely believe it because I haven’t had any illnesses. I don’t have high blood pressure…high cholesterol, diabetes,” she told US newspaper the New Jersey journal in November.
Ms Borders was only in her first month at the World Trade Centre One, where she worked on the 81 floor, when the bombers flew into the building. Despite orders from her supervisor to stay at her desk, the then-28-year-old’s disobedience saved her life as she made it out of the building.…
She was diagnosed with cancer in 2014 and started a course of treatment. Independent UK

She managed to make it down to the ground level, and was walking away when the second plane struck the tower, leaving her covered from head to foot in thick grey dust. Telegraph
VIDEO: Marcy Borders Dust Lady dead Dailymotion
_____________________________________________________________
From CBS Local:
High School Students Study ‘Cancer Alley’ Near Fresh Kills Landfill
Research: 11 Percent More Cancer Deaths On Staten Island Than Rest Of City
May 16, 2013 2:35 PM

“The thing is since Staten Island is notorious for having one of the single largest landfills on the eastern seaboard – the Fresh Kills Landfill – we hypothesize that these dangerous fungi do exist in harmful concentrations on the island,” she said.
So, landfills are conducive to growing lots of bad fungi?
“Unfortunately, yes,” she said.
So, what does that mean if you live near the former Fresh Kills Landfill?
“If you live in that area and you are immunocompromised, which means that you have a weakened immune system or some sort of prevailing illness – and this could range anywhere from asthma to allergies and all the way up to cancer and chemotherapy – you are susceptible to having complications due to these spores,” Colossi said.
So, what is a person to do, stay inside and close the windows?
“We recommend that you put in some sort of air purification system and we also recommend that you keep your medication with you readily available just in case anything were to happen because we can’t force anyone to move and leave their homes, but we would like to make people aware of this health risk,” he said.
But it really is that bad around the landfill?
“That it is, especially where there’s a spot right above it that is termed ‘cancer alley’ because it has such high mortality rates due to cancer there,” he said.
Colossi said he knows people who have been sickened.
“Apparently, 30 percent more people die of heart disease on Staten Island than the rest of the city as a whole and 11 percent more people die of cancer than the rest of the city,” he said.
He said anywhere between “some” and “most of it” could be due to the spores.
With Fresh Kills closed, is the danger subsiding?
“Unfortunately, no,” said Simineri. “You can still the rot and decaying matter just sitting there, just rotting away, which is perfect for fungal growth, unfortunately.”
If this is a public health hazard, which the research suggests, should the city do something? Is there something that can be done?
“One thing that I’ve noticed was that some other landfills have coverings, although we’re not really sure if that would actually make much of an impact,” she said. “The one thing that we’re looking into are fungicides. So, although there is no way to completely eradicate the fungi from the area, which would also be detrimental to the ecosystem since they are, naturally, a part of it, we would just like to use fungicides to get the population down.”
We checked records from the city health department and they confirm “a relatively slight, but statistically significant, elevation of certain cancers on Staten Island compared with the rest of the city.”
Colossi added that the field is so unexplored and so little is known about it that the United States actually doesn’t have standards for what is a safe amount to inhale and what is not.
“So, ended up having to look at a European model for that and we were able to determine, by those standards, that these were dangerously high amounts,” he said.
Why did they suspect Fresh Kills?
“Because it is the perfect source of decaying matter, which these decomposers feed off of,” he said. “It’s basically a perfect nutrient source.”
_______________________________________________________

Eastern New Jersey is “Cancer Alley” – radioactive fallout affecting New Jersey?
The radioactive dust cloud would have swept over New Jersey on September 11 and in the days, weeks and months following the attacks. The fallout from the attacks would have also come from Staten Island, which is located adjacent to eastern New Jersey as the map above shows. The townships of Woodbridge Township, Elizabeth, Perth Amboy and Linden would have all been affected by the radioactive dust particles in the atmosphere that came from Fresh Kills and continued to drift from the WTC site.
Book Singleton: Never Cross a Jersey Girl:
“… eastern New Jersey being labeled Cancer Alley, was somehow linked to the humongous landfill. The residents of Linden and Carteret, directly across the bay in New Jersey, could actually see the residue of Fresh Kills incinerators descending on their property during rainfalls. When the ash didn’t blow out to the Atlantic Ocean, it coated abutting New Jersey communities like toxic dandruff.”
_________________________________________________________
From Wastedive:
New York ‘Cancer Alley’ study could mean prize for high schoolers

Dive summary:
Two Staten Island high school seniors have been researching an area known as “Cancer Alley” near Fresh Kills Landfill in New York.
The students say fungal spores around the landfill could be connected to the 11% higher rate of fatal cancer and 30% increase in heart disease from other nearby areas.
Fresh Kills Landfills is one of the largest landfills on the eastern seaboard, and while the landfill is now closed, the spores continue to grow as the trash decomposes.
From the article:
“The thing is since Staten Island is notorious for having one of the single largest landfills on the eastern seaboard – the Fresh Kills Landfill – we hypothesize that these dangerous fungi do exist in harmful concentrations on the island,” she said.
So, landfills are conducive to growing lots of bad fungi?
“Unfortunately, yes,” she said. …
________________________________________________________________

From SI Live:
The Island’s tragic breast cancer mystery
By DEBORAH YOUNG on October 04, 2009 at 7:00 AM, updated October 04, 2009 at 1:29 PM
Hammel/Staten Island AdvanceStaten Island has the highest breast cancer mortality rate in the city.
STATEN ISLAND, N.Y. — My mother, my aunt, my neighbor, sister, daughter, grandmother, teacher, friend.
The stories are told every day on Staten Island in pained and quiet voices: Who was diagnosed with breast cancer, who is going through treatment, who died after battling the disease.
Lives get lost to breast cancer far more often in this borough than in the rest of the city, and at a higher rate than most of the state and nation.
In fact, according to the state Department of Health, the mortality rate from the disease here is higher even than in the Long Island counties that have come to symbolize the scourge — spotlighted by national media, named in congressional acts and given millions of research dollars to root out the cause.
Trying to unravel the mystery on Staten Island is a small band of passionate researchers at the College of Staten Island in Willowbrook.
For the past two years, scientists at the Staten Island Breast Cancer Research Initiative have been engaged in groundbreaking work — plotting the demographics of the disease, performing sophisticated lab testing on chemicals in the environment and educating women in the community — all on a shoestring budget.
“All we need to know is why here,” said Dr. Donna Gerstle, the director of the initiative and of the Center for Environmental Science at CSI. “Staten Island has the highest breast cancer mortality rate in the five boroughs for at least 20 years, and everything we’re doing is to find out why.”
Every year, about 335 Staten Island women are diagnosed with breast cancer, and 77 women die of the illness, according to statistics gathered between 2002 to 2006 by the state Department of Health.
The incidence of the disease here is among the highest in the state; and the mortality rate of 27.7 per 100,000 women represents a peak.
“There is a stunningly high correlation between the length of residency and incidence of breast cancer,” said Dr. Gerstle, herself a native Islander, living in West Brighton.
CLUES IN OBITUARIES
The researchers utilize a rich source of information unique to this borough — Staten Island Advance obituaries.
Control groups are created, and death certificates of women who died of breast cancer are compared with their obituaries to learn about where they lived, especially during key times for breast tissue development, such as puberty.
So far, more than 10,000 obituaries from 1980 to 1990 have been analyzed; funding provided last year by the City Council is allowing the team to keep going through the year 2006.
Indeed, the research has confirmed there is a higher rate of breast cancer among women who live in neighborhoods near the former Fresh Kills Landfill and the Island’s Super Fund sites — but the scientists balked at pointing to more specifics.
“Staten Island is the cluster,” said Dr. Alfred Levine, arguably the patriarch of the Center for Environmental Science, who taught Dr. Gerstle when she was a graduate student. “Everywhere you look.”
And the information in the obituaries threw up another puzzle: Socio-economic issues like low educational level, which often predict poor medical care, and, as a result, higher mortality rates, just didn’t factor in to the equation on the Island.
“The numbers are scary,” said Councilman James Oddo (R- Mid-Island).
Oddo and Council Speaker Christine Quinn awarded $140,000 in the past two fiscal years for the study, providing much of the budget for the initiative, which also receives state money and private awards, but operates on less than $100,000 a year.
“We owe it to the women of Staten Island to find out what it is, and if there is a way to avoid it, whether it is personal behavior or it is the environment,” the councilman added.
Oddo cited the long wait time for a mammography in the borough — which has been somewhat ameliorated in recent years by two new mammography machines — as one systemic health-care failing here that could play a role in the deaths.
“That might be part of it, but why should we be higher than the South Bronx?” said Dr. Gerstle. “There has to be more to it.”
TOXINS PLAY A ROLE
So is the brand of breast cancer that strikes in the borough particularly vicious, killing women before they have a chance to beat it?
Might the industrial landscape trigger the mortality from breast cancer here, and also have a role in the borough’s rates of lung cancer and lymphoma, which are also the highest in the city?
In fact, the scientists said, this study initially focused on lung cancer, because the Island has long been known as an epicenter of that disease. But after pouring over data, it became obvious that breast cancer deaths here are the shocker.
“The minute we started looking at breast cancer, the results hit us in the face,” said Levine. “The statistical significance of the results made it in no way this could be pure chance.”
Enter Dr. Jimmie Fata from the University of California at Berkeley, who joined the Island research team and designed a way to mimic mammary tissue at puberty.
In the lab, he tests carcinogens commonly found here in the environment.
But what makes his work different than other studies, is he is looking for the tipping point, the concentrations of these chemicals where tissue begins to change.
A paper he and a graduate student will present at a conference in November will share one hypothesis produced by their early research: It asks, might the high average concentration of benzene here, which is 88 times the benchmark level, be linked to the breast cancer mortality rate?
These kinds of questions have haunted Pamela Silano ever since her mother died of fast-spreading breast cancer in 1993. At least one person in almost every house on her short block in Meiers Corners died of cancer, she said.
“We always heard the stories about the landfill and Newark’s pollution affecting the Island and the people. Each time someone would pass away from cancer, the families would always say it was the landfill or the fumes that blew over,” she said. “But, I guess, when you’re grieving you have to blame it on someone, right? At least that is what I thought until it happened to my family.”
This kind of pattern — with so many cancer deaths in such a short block — could be a fluke, a statistical anomaly, ventured Dr. Gerstle, who, as a scientist, is wary of drawing conclusions without data to prove them.
But it is the quest for an explanation that is driving the long, exhaustive hours the researchers spend at work.
“These are my relatives, my friends, I understand,” said Dr. Gerstle, shaking her head and looking down. “We’re trying to do the best we can for Staten Islanders. We hope we find an answer one way or another. We won’t give up until we do.”
_________________________________________________________________
Centers for Disease Control and Prevention WTC Health Program – at a glance (December 2016)
Link: CDC–World Health Center Health Program
Download pdf: World Trade Center Health Program
Enrollment in the WTC Health Program:

New enrollees past 24 months

New enrollees responders and survivors past 12 months

WTC Health Program enrollment by state

Members with certifications by Zadroga Act – categories of conditions
Top 10 Certified Conditions
Members with certifications – age distributions

Members with aerodigestive certifications – age distribution

Members with musculoskeletal certifications – age distribution

Members with mental health certifications – age distribution

Number of members with only the number of certifications

Previous reports
Previously Reported Information
Links:
- Data as of September 2016
(16 pages, 500 KB) - Data as of June 2016
(11 pages, 714KB) - Data as of February 2015
(4 page, 169KB) - December 20, 2014
(4 page, 729KB)
________________________________________________________________
WTC Health Program
The World Trade Center Health Program (WTC Health Program) provides medical benefits to individuals affected by the September 11, 2001 terrorist attacks on the United States.[1] The WTC Health Program was established by Title I of the James Zadroga 9/11 Health and Compensation Act of 2010 (Zadroga Act), P.L. 111-347, which amended the Public Health Service Act. The United States Congress passed the bill in December 2010 and United States President Barack Obama signed it into law on January 2, 2011.[2] The Zadroga Act required the WTC Health Program to begin administering medical benefits on July 1, 2011. On December 18, 2015, the Zadroga Act was reauthorized to provide medical benefits to affected individuals until 2090.[3] The National Institute for Occupational Safety and Health (NIOSH), within the Centers for Disease Control and Prevention, administers the program. The Centers for Disease Control and Prevention is component of the United States Department of Health and Human Services (HHS). Wikipedia
___________________________________________________


